
Pre-implant surgery
Pre-implant analysis
At your request, a surgical guide can be produced from the systematic scan analysis we carry out before placing your implants. This guide allows us to fix the implants very precisely in the position defined by the X-ray without the need for a visual approach to the bone volume. As a result, no incision is necessary, as the guide is fixed to your gum after a simple local anaesthetic.
The placement of dental implants requires thorough preparation, carried out prior to the operation with the help of examinations such as X-rays, scans, etc. The placement of dental implants can be exposed to the problem of insufficient bone capital in some patients. In order to guarantee effective anchorage and durability for the future prosthesis, dental implants must be placed in sufficient bone volume.
When bone volume is too low, it can be surgically increased by a bone graft or bone filling. The grafted bone can either come from the patient: this is called an autograft, and is generally taken from the lower jaw; or it can come from a biomaterial: this is called a non-grafted graft.
A preliminary bone assessment is imperative to define the technique, the volume of bone to be reconstructed and whether or not dental implants should be placed simultaneously.
Bone grafting will only be used as a last resort, if the shortest dental implants cannot be used. The latest scientific and technological advances mean that bone grafting can be avoided or reduced in the majority of cases.
Pre-implant surgery
Pre-implant bone grafting
Autografting
The bone is taken from the person receiving the graft, usually in the lower jaw, either in the chin area or on the sides. We will be able to recover a small block of bone, which will be stabilised using a miniscrew. This type of graft is called an apposition or onlay graft.
A healing period of 6 to 8 months is usually required for the graft to integrate. The implants can then be inserted and the fixing screws usually removed at the same time. This type of bone graft can be used to treat bone defects that are extensive in both height and thickness, under a simple local anaesthetic.
For patients with very significant bone loss who require larger grafts, bone can be taken from the skull or hip. These grafts are the responsibility of maxillofacial surgery. They are performed under general anaesthetic in hospital.
Allografts
The bone block is no longer taken from the patient, but comes from a living donor bank. These materials undergo a series of sanitary treatments to ensure that they are extremely safe to use. Bone banks are accredited by the ANSM.
This type of bone graft is used to treat bone defects that are very extensive in height and thickness. This long and meticulous operation can be carried out under conscious sedation for your comfort.
Xenograft
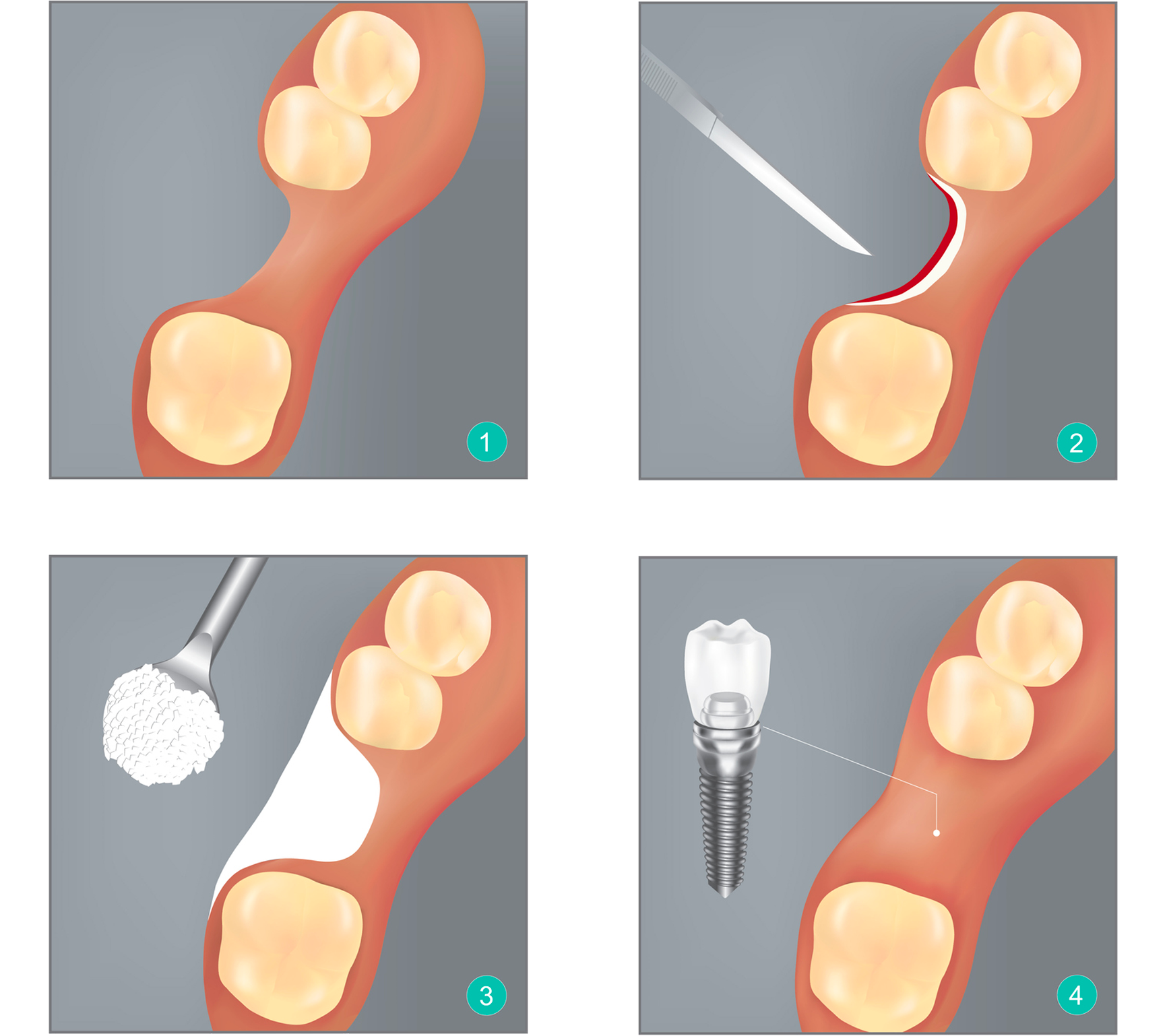
In this situation, the bone defect is filled with various biomaterials of animal origin (bovine, porcine, equine). In all cases, these materials undergo a series of sanitary treatments to ensure that they are extremely safe to use. The graft is placed in the area where the lack of bone poses a problem. Once immobilised, it is gradually immobilised by a membrane of animal collagen, and gradually guides new bone formation.
This type of bone filling may be combined with simultaneous or deferred placement of dental implants. A healing period of 4 to 9 months is necessary for optimal consolidation of the graft. This bone addition compensates for small defects, filling of extraction sockets and lack of bone volume in the sub-sinus area.
Pre-implant surgery
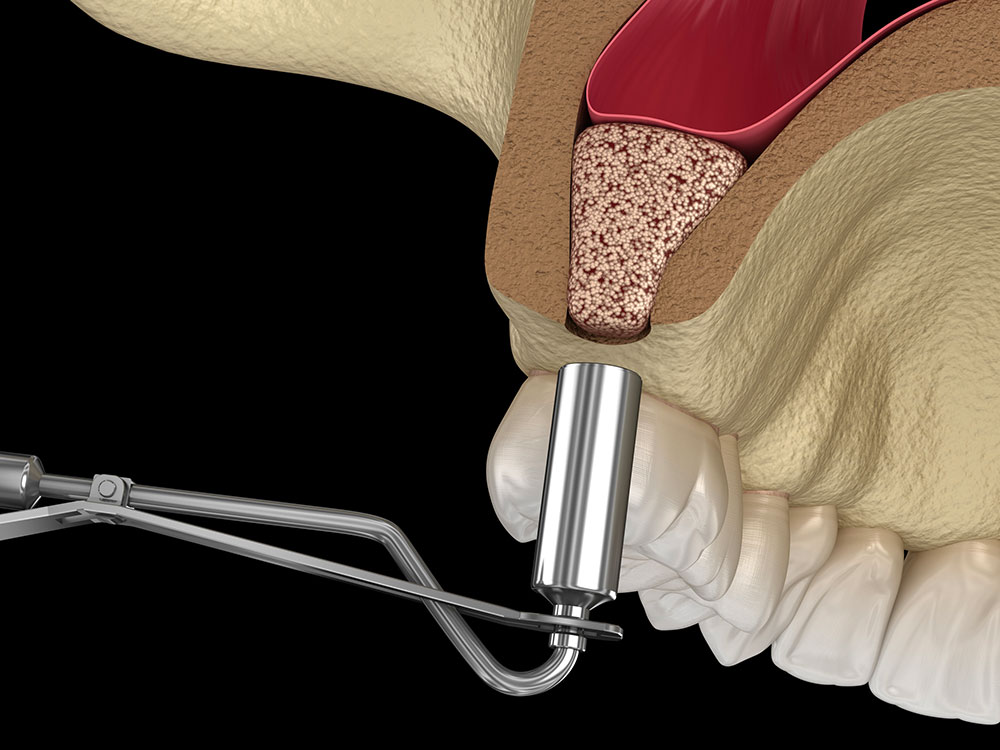
Sinus-Lift
In the posterior sectors of the maxilla, in edentulous areas, there is often an increase in sinus volume (posterior cavity) at the expense of the bone crest.
The volume occupied by the bone gradually diminishes. The sinuses then occupy the space left empty by the disappearance of the bone.
There are two possible scenarios:
- Either the height of the crest is at least 6 mm and short dental implants can be placed with a real success rate.
- Or the height of the crest is less than 6 mm: it is then necessary to increase the volume of the bone crest at the expense of the sinus, to position dental implants with a more common length (13mm).
Sinus surgery and dental implants are performed in the same session, so that patients do not have to undergo pre-medication, post-operative consequences and two operations twice.
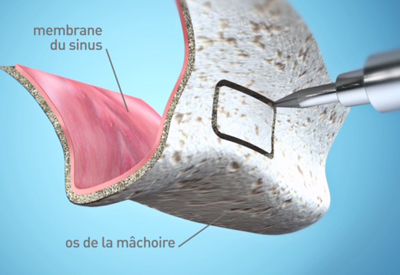
A flap is placed on the anterior surface of the sinus.
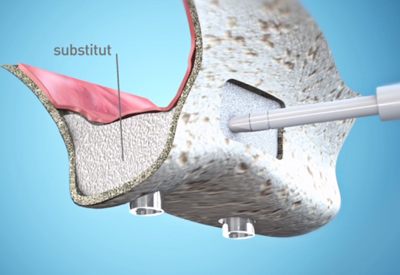
In the majority of cases, it is necessary to fill in and increase the bone volume of this space with a substitute, in order to allow the dental implants to be firmly and permanently anchored.
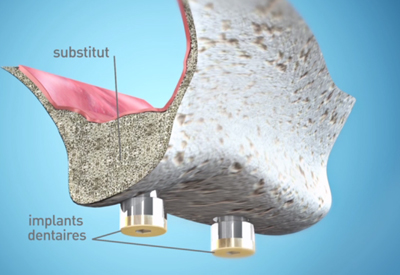
Where possible, this pre-implant surgery can be carried out at the same time as the placement of dental implants. This considerably reduces the operating time and the duration of the treatment.
Pre-implant surgery
Guided bone regeneration
Guided bone regeneration is a set of surgical techniques designed to regenerate a volume of bone by stimulating the production of bone using a membrane.
The technique
The surgical protocol consists of isolating the bone defect using a membrane, so that the volume created is gradually filled by new bone. The membrane prevents the gum from colonising the bone defect. It is then necessary to wait 4 to 9 months for healing before the implant can be placed. Sometimes, this technique can be used at the same time as implant surgery, for example when a tooth is extracted and the implant placed immediately. The guided bone regeneration technique is reserved for the reconstruction of small volumes of bone. For larger reconstructions, the dental surgeon has to use bone grafts, taking large volumes from the mouth or skull.
Regeneration materials
A distinction is made between resorbable membranes, which are ‘dissolved’ after a few weeks, and non-absorbable membranes, which have to be removed during a second operation. In addition, the membrane can be combined with the placement of small amounts of bone taken from elsewhere in the mouth or with the use of bone substitutes.
What are the possible complications?
For guided bone regeneration to be successful, the membrane must be completely covered by the gum. In some cases, healing does not take place as expected and the membrane is exposed to saliva. Infection of the operated area may then occur and compromise the result of the operation. More generally, as after any operation, there may be a haematoma, oedema, inflammation and temporary pain.
Risk factors
The guided bone regeneration technique is reliable for reconstructing small volumes of bone. In smokers, healing is very disturbed and failures are more frequent.